
Page 12 - Construction Forms
P. 12
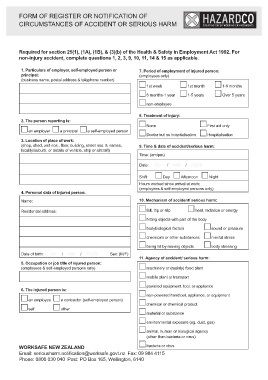
FORM OF REGISTER OR NOTIFICATION OF TM
CIRCUMSTANCES OF ACCIDENT OR SERIOUS HARM
Required for section 25(1), (1A), (1B), & (3)(b) of the Health & Safety in Employment Act 1992. For
non-injury accident, complete questions 1, 2, 3, 9, 10, 11, 14 & 15 as applicable.
1. Particulars of employer, self-employed person or 7. Period of employment of injured person:
principal: (employees only)
(business name, postal address & telephone number)
1st week 1st month 1-6 months
6 months-1 year 1-5 years Over 5 years
non-employee
2. The person reporting is: 8. Treatment of injury: First aid only
None Hospitalisation
an employer a principal a self-employed person Doctor but no hospitalisation
3. Location of place of work: 9. Time & date of accident/serious harm:
(shop, shed, unit nos., floor, building, street nos. & names, Time: (am/pm)
locality/suburb, or details of vehicle, ship or aircraft) Date: DD / MM / YEAR
Shift: Day Afternoon Night
4. Personal data of injured person: Hours worked since arrival at work:
Name: (employees & self-employed persons only)
10. Mechanism of accident/ serious harm:
Residential address: fall, trip or slip heat, radiation or energy
hitting objects with part of the body
bodybiological factors sound or pressure
chemicals or other substances mental stress
being hit by moving objects body stressing
Date of birth: DD / MM / YEAR Sex: (M/F) 11. Agency of accident/ serious harm:
machinery or (mainly) fixed plant
5. Occupation or job title of injured person:
(employees & self-employed persons only)
mobile plant or transport
6. The injured person is: powered equipment, tool, or appliance
non-powered handtool, appliance, or equipment
an employee a contractor (self-employed person) chemical or chemical product
self other material or substance
environmental exposure (eg. dust, gas)
animal, human or biological agency
(other than bacteria or virus)
WORKSAFE NEW ZEALAND bacteria or virus
Email: seriousharm.notification@worksafe.govt.nz Fax: 09 984 4115
Phone: 0800 030 040 Post: PO Box 165, Wellington, 6140